| Colon Prep without Fasting and
the Harsh Chemicals to evacuate the colon?
Yes, now there is a better and safer solution for prepping
patients for any type of colon examinations. Much, much higher
patient compliance and patient/physician satisfaction.
Dr. David Graham, a member of our medical advisory board,
who is considered one of the nation's top fifty most influential
Gastroenterologists and Dr. Kamran Ayub, headed a recent
study. This was a small study based on proving the efficacy
and desirability for the patient/physician with the colonoscopy
prep. All work was done at the VA Hospital, Houston.
______________________________________________________________________________________________________
Digestive Disease Week April 2000, Part 2 · Volume 51 · Number 4
*3423 PULSED IRRIGATION EVACUATION: A BETTER TECHNIQUE FOR COLON CLEANSING?
Kamran Ayub, Waqar Quershi, Rosetta Brown,
Rhonda A. Cole, David Y. Graham
VA Med Ctr, Houston, TX.
Background: The first, and possibly most critical, step
in colonoscopy is to have an adequately prepared colon. Unfortunately,
none of the currently used colon cleansing regimens are completely
satisfactory both in terms of patient complaints of unpleasant
side effects and in terms of failure to provide a clean colon.
The failure rate with traditional preparation is typically
10 to 30 %. We used the Pulsed Irrigation Evacuation (PIE)
device for colon cleansing. This device administers warm
tap water through a cuffed speculum with microprocessor-timed
pulses of inflow and outflow. The rehydrated fecal matter
is collected in a closed system that is discarded. The PIE
technique is FDA approved for the management of fecal impaction.
We hypothesized that use of PIE should result in rapid colon
cleansing for colonoscopy with minimal patient discomfort.
Methods: Consecutive outpatients scheduled for colonoscopy
were offered the opportunity to participate. Main exclusion
criteria were suspected bowel obstruction, previous colon
resection, and severe congestive heart failure.
Patients were advised to take clear liquids after 1 PM on
the day prior to examination, one bottle of magnesium citrate
(165 ml) the evening prior to examination and were kept NPO
after midnight. Upon arrival to the Endoscopy suite, PIE
was performed until the return was clear, followed by colonoscopy.
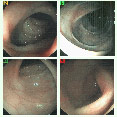
Endoscopic photographs were taken in each segment of the
colon, and video recordings were made. Patient discomfort
during colon cleansing was assessed by a questionnaire. The
quality of colon cleansing was graded using a previously
used scoring system during the procedure. Two Endoscopists
also independently graded the quality of colon cleansing
based on the photographs/video.
Results: 20 consecutive patients participated (mean age
= 60 yr - range of 45-80 yr). PIE was well tolerated. The
only side effect was mild abdominal cramps during large pulses.
Colonoscopy preparation was complete to the cecum or terminal
ileum in all.
Colon cleansing was graded as acceptable or better in all
(100% success: excellent = 4 patients, good = 15 patients,
acceptable = 1 patient). The average time for cleansing was
25 minutes (range 20 to 35) and typically, approximately
6 gallons of water was required. Five patients had previous
colonoscopy with GoLytely preparation and all preferred PIE.
Conclusions: PIE Prep results in optimal and rapid colon
cleansing while causing minimal patient discomfort. It could
be used as a primary colon preparation or for same day cleansing
of those with poor traditional preparation.
The results indicated that there was no comparison between
the PIE* Prep and the traditional means. Our method was
accepted much higher for both the patient/physician.
A much larger study with Dr. David Graham is being funded
by the "American College of Gastroenterology".
In this much larger study the Medical team is comparing
Golytley, Phosphosoda, the traditional chemical Colon prep,
against the PIE* Prep and comparing their effectiveness and
patient satisfaction. Dr. Graham reports a total of 80 patients
have been completed so far with PIE Prep showing excellent
results over the chemical methods. Dr. Graham intends to
include 500 patients and expects to have it completed by
December 2001.
How is the PIE* Prep performed?
The patient is scheduled for the colonoscopy. The night
before the colonoscopy, they are instructed to take two tablespoons
of Milk of Magnesia. Then the patient arrives at the Gastroenterologist
office one hour early. A nurse, using the PIE* System, has
the patient to lie on a table and the PIE* Speculum is inserted
into the rectum.
The speculum is designed to inflate and fill the rectal vault.
Then the computer driven PIE* System begins infusing small
quantities of water with the water being rapidly pulsed to
break up and clean the entire colon area. The quantities
of water are increased so that the entire colon can be cleaned
up to the ileocecal valve.
The procedure typically takes about 30-45 minutes!
Is the PIE* Procedure comfortable to the patient?
Yes. In
fact many of the patients find the procedure so relaxing
that they fall asleep.
In fact, the patient experiences no ill effects and can
usually return to their normal activities immediately after
the colonoscopy.
Is the PIE* Prep always successful?
Yes. There's never been
a failed PIE* Prep.
It is the PIE* Prep always reimbursable?
No. We are being
issued a CPT Code in January 2002 for fecal impaction removal
without anesthesia. We're working to have the AMA also modify
this code or to establish a separate Code for Colonoscopy
Prep.
Patients will pay out of their own pocket.
We believe that there are many patients who dislike the
traditional oral prep so much that they will pay out of their
pocket for this alternative. From a recent survey, we found
over 50%, when given an alternative, would gladly pay out
of their pocket.
What if they patient arrives at the Gastroenterologist office
and has used traditional oral prep and is not clean, can
the PIE* Prep solve this problem?
Absolutely, with a PIE* System in your office, the patient
can remain on your colonoscopy table and in only a few minutes
be totally clean.
You are now able to maintain their scheduled appointment
about rescheduling.
Many Gastroenterologist have told us that some of their
patients absolutely refused to reschedule and go through
the oral prep again. Plus, keeping the appointment for the
Gastroenterologist means that the schedule appointment was
not lost.
|